A
B
C
D
E
F
G
H
I
J
K
L
M
N
O
P
Q
R
S
T
U
V
W
X
Y
Z
Click a letter to see a list of conditions beginning with that letter.
Click 'Topic Index' to return to the index for the current topic.
Click 'Library Index' to return to the listing of all topics.
When Your Child Has Hirschsprung Disease
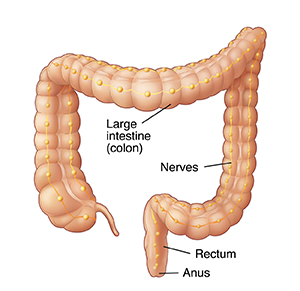
The colon (large intestine) holds stool (waste) left in the body after digestion. The colon is lined with nerves. These tell the colon when to contract (squeeze) and relax (open). The colon contracts and relaxes to push stool into the rectum. Stool leaves the rectum through the anus. In a child with Hirschsprung disease, nerves are missing in the anus and rectum and in part or all of the colon. The part of the colon without nerves can’t relax. So, stool can’t leave the body.
Types of Hirschsprung disease
Hirschsprung disease is categorized based on how much colon is affected. Your child’s healthcare provider can tell you which type of Hirschsprung disease your child has. Types of Hirschsprung disease include:
-
Ultrashort segment: Nerves are missing from a very small portion of the rectum.
-
Short segment: Nerves are missing from the rectum and a small portion of the colon.
-
Long segment: Nerves are missing from the rectum and a larger portion of the colon.
-
Very long segment: Nerves are missing from the entire colon and rectum and sometimes part of the small intestine.
What are the signs of Hirschsprung disease?
Hirschsprung disease is most often diagnosed in newborn babies—the most common sign is not passing stool within the first 24 to 48 hours of life. Other signs in newborns can include swelling of the abdomen, vomiting, and fever. In some cases, the problem doesn’t cause signs or symptoms until the child is a little older. When this happens, signs of a problem include constipation (hard, dry stool that can be hard to pass), poor appetite, poor weight gain, and not growing as much as normal.
How is Hirschsprung disease diagnosed?
First, your healthcare provider will take a health history, ask about symptoms, and do a physical exam. These help find the cause of the problem. The following tests may then be done:
-
Barium enema. A chalky liquid containing barium is inserted through the anus into the rectum. This liquid coats the inside of the colon and lower part of the small intestine so they show up on an X-ray. The X-ray shows if the colon and lower part of the small intestine are blocked by backed-up stool. In some cases, a substance other than barium may be used, but the test is done in the same way.
-
Rectal biopsy. A small tube is inserted through the anus into the rectum. Through this tube, a tiny amount of tissue is removed. The tissue is studied in the lab. In some cases, a larger amount of tissue is taken with a surgical biopsy. If no nerves are found in the tissue, it's a sign of Hirschsprung disease.
-
Anorectal manometry. A tube with a small balloon on its tip is inserted through the anus into the rectum. The balloon is then inflated. Normally, the balloon would stimulate nerves in the colon, causing the colon to relax and open. With Hirschsprung disease, the colon contracts and closes instead.
How is Hirschsprung disease treated?
Hirschsprung disease is treated with surgery. The section of colon without nerves is removed. The healthy ends of the colon are then reconnected. This surgery is called bowel resection.
If your child needs a stoma
Your child may need a stoma before or after surgery. This provides a new way for waste to leave the body. A small opening is made in the abdomen. This opening is connected to the colon. Waste leaves the body through this opening and empties into a bag. The stoma may be temporary or permanent, depending on how much of the colon is affected by Hirschsprung disease. If your child needs a stoma, your healthcare provider will tell you more about it. Sometimes a stoma is placed temporarily and a follow-up surgery is planned to reconnect the remaining portion of bowel at a later time.
What are the long-term concerns?
If a large portion of the colon must be removed, your child may have long-term digestive problems. But in general, most children with Hirschsprung disease do very well after surgery. Even so, your child’s bowel movements may not be normal. Hirschsprung disease can cause the rectum and anus to collapse. If so, stool can’t be pushed out normally. This can result in minor problems such as constipation and leakage. These problems are often treated with medicine and a high-fiber diet. Also, children with Hirschsprung are more likely to develop an infection of the colon (enterocolitis). Your child’s healthcare provider can tell you more about your child’s situation.
Online Medical Reviewer:
Jen Lehrer MD
Online Medical Reviewer:
L Renee Watson MSN RN
Online Medical Reviewer:
Rita Sather RN
Date Last Reviewed:
5/1/2022
© 2000-2024 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare professional's instructions.